最近の医学論文 後編
【前編】より
⑮BE-FAST (Balance, Eyes, Face, Arm, Speech, Time): Reducing the Proportion of Strokes Missed Using the FAST Mnemonic. (2017.1.12 published online)
脳卒中の早期発見の啓蒙活動に、海外では FASTをよく用いる。これは、Face, Arm, Speechの略で、これらの異常があれば脳卒中の可能性があるとするもの。ただし、これでは 14.1%を見逃してしまう。そこで、Balance, Eyesという、バランスの異常と視覚症状を加えると、見逃しが 4.4%に減少するのではないかという報告。
BE-FASTだとゴロが良いので、脳卒中早期発見の啓蒙に使えるのではないかと思う。ただ、バランスの異常は、発熱でふらついていても起こりそうだから、特異度は低くなりそうだけれど・・・。
⑯Incidence and outcome of functional stroke mimics admitted to a hyperacute stroke unit. (2016.8.28 published online)
脳卒中と誤診されるような紛らわしい病態を stroke mimicsと呼ぶ。脳卒中としてロンドンの超急性期脳卒中ユニットに入院した症例 1165名を対象に、stroke mimicsについて調べた。実際に脳卒中だったのは 904名 (77.6%)、medical mimicsは 163名 (14%)、functional mimics (≒心因性) は 98名 (8.4%) だった。Medical mimicsでは過去の脳卒中による機能障害、てんかん、片頭痛などが多かった。
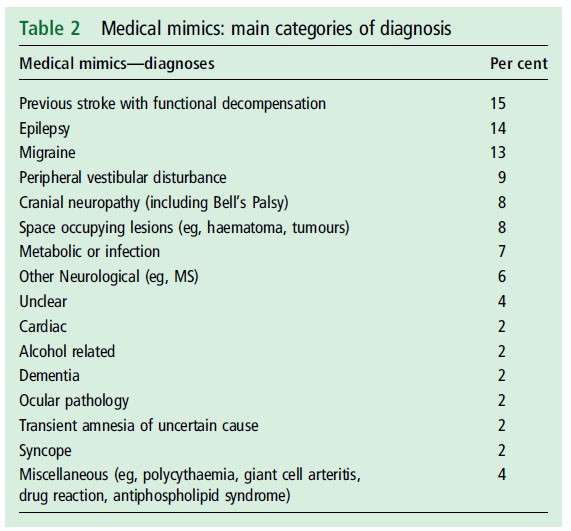
medical mimics
こんなに心因性って多いのかなぁ・・・とも感じるけれど、著者らの所属に “Department of Neuropsychiatry” “Institute of Psychiatry, Psychology and Neuroscience” というのがあるので、精神疾患を持つ患者のかかりつけが多いのかもしれない。
⑰Impact of Rehabilitation on Outcomes in Patients With Ischemic Stroke: A Nationwide Retrospective Cohort Study in Japan. (2017.1.20 published online)
虚血性脳卒中で入院した患者のリハビリ効果を調べるために、データベースを用いて 100719名を解析。リハビリ早期開始 (入院後 3日以内)、リハビリ強度 (単位数) について、Barthel index改善の有無を評価。早期開始による Barthel indexの改善は odds ratio 1.08 (95%信頼区間 1.04~1.13), 強化リハビリ療法 > 5単位/dayによる Barthel indexの改善は odds ratio 1.87 (95%信頼区間 1.69~2.07) であった。
解析に用いた数が大きいので有意差自体は出やすくなっている。しかし Barthel indexの改善に対する Odds比 1.08とか、リハビリを早期に始めるメリットって、この程度なのかと思った。一方で、リハビリ強度については、綺麗な量相関関係があり、しっかりとリハビリは頑張った方が良さそうだ。
⑱YAMATO Study (Tissue-Type Plasminogen Activator and Edaravone Combination Therapy). (2017.1.24 published online)
日本からの報告。血栓溶解療法の前にエダラボンを投与しても、後にエダラボンを投与しても、再開通率や症候性脳卒中、mRSでの転帰に有意差はなかった。
個人的には、エダラボンの効果自体が微妙だと思っている (全くゼロじゃないだろうけれど、薬価に見合うだけのことはないのでは・・・) ので、予想範囲内の結論。エダラボンが本当に有効なのかについて、これまでの臨床試験はベースラインが揃っていなかったり、ブラインド化されていなかったりするので、きちんとしたデザインの RCTが行われることの方に関心がある。
⑲Abstract 18462: Proton Pump Inhibitor Use Increases the Associated Risk of First-Time Ischemic Stroke. A Nationwide Cohort Study (2016.11.11 published online)
プロトンポンプ阻害薬 (PPI) が脳梗塞のリスクを高める (incidence rate ratio (IRR) of 1.21 (95% CI 1.16-1.27; P-value <0.0001)) という報告。
元々、AHA/ASA虚血性脳卒中予防ガイドライン2014の 2195ページには “Recently, evidence has emerged that proton pump inhibitors (PPIs), such as esomeprazole, may reduce the effectiveness of clopidogrel. However, a large population study from Denmark suggested that PPIs themselves may increase the risk of cardiovascular events, so that when they are used with clopidogrel, the PPI may be the culprit.” という記載があり、PPIで心血管イベントが増えるかもしれないとされていたけれど、それを裏付ける結果。最近、PPIの副作用についての論文が増えている。
FDAより、NOACsで血管炎の恐れとの安全情報。
プラザキサとリポバスの併用で、出血リスクが高まる (OR 1.46[1.17-1.82]) らしい。詳細はリンク先のブログ記事参照。
㉒Warfarin–Associated Nonuremic Calciphylaxis. (2017.1.11 published online)
ワルファリンに関連した非尿毒症性 Calciphylaxisの報告。著者らの 3例に加えて、15例の文献的検討。Calciphylaxisは腎不全に関連して起こることが近年話題になっているが、腎不全がなくてもワルファリン内服に関連して発症することが極めて稀ながらあるらしい。治療は抗凝固療法やチオ硫酸ナトリウム (デトキソール) などが用いられ、18例中 15例が生存した。古典的 Calciphylaxisの死亡率が 50~80%とされているのと比較すると予後は良好だった。
Facebookでこの論文について書いたら、リウマチ科医の先生から「vasculitis mimicsとして有名」と教えて頂いた。
㉓Pharmacologic Treatment of Hypertension in Adults Aged 60 Years or Older to Higher Versus Lower Blood Pressure Targets: A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians. (2017.1.17 published online)
アメリカ内科学会とアメリカ家庭医学会より、高齢者の血圧管理についてのガイドラインが公表された。GRADEシステムで作成されている。
Recommendation 1:ACP and AAFP recommend that clinicians initiate treatment in adults aged 60 years or older with systolic blood pressure persistently at or above 150 mm Hg to achieve a target systolic blood pressure of less than 150 mm Hg to reduce the risk for mortality, stroke, and cardiac events. (Grade: strong recommendation, high-quality evidence). ACP and AAFP recommend that clinicians select the treatment goals for adults aged 60 years or older based on a periodic discussion of the benefits and harms of specific blood pressure targets with the patient. Recommendation 2:ACP and AAFP recommend that clinicians consider initiating or intensifying pharmacologic treatment in adults aged 60 years or older with a history of stroke or transient ischemic attack to achieve a target systolic blood pressure of less than 140 mm Hg to reduce the risk for recurrent stroke. (Grade: weak recommendation, moderate-quality evidence). ACP and AAFP recommend that clinicians select the treatment goals for adults aged 60 years or older based on a periodic discussion of the benefits and harms of specific blood pressure targets with the patient. Recommendation 3:ACP and AAFP recommend that clinicians consider initiating or intensifying pharmacologic treatment in some adults aged 60 years or older at high cardiovascular risk, based on individualized assessment, to achieve a target systolic blood pressure of less than 140 mm Hg to reduce the risk for stroke or cardiac events. (Grade: weak recommendation, low-quality evidence). ACP and AAFP recommend that clinicians select the treatment goals for adults aged 60 years or older based on a periodic discussion of the benefits and harms of specific blood pressure targets with the patient.
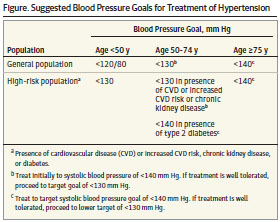
降圧基準の提案 (JAMA)
㉕Management of Sepsis and Septic Shock. (2017.1.19 published online)
敗血症の治療ガイドラインである Surviving Sepsis Campaignが改定された。主要な推奨項目は下記 (抜粋)。
・敗血症と認識してから 1時間以内に、想定される病原体を全てカバーした広域抗菌薬を投与。
・解剖学的な感染源のコントロールを可能な限り速やかに行う。
・毎日、培養結果や臨床的改善を基に抗菌薬を de-escaltionすることを検討。
・敗血症性の低血圧がある場合、3時間以内に 30 ml/kgの晶質液を輸液。
・昇圧剤を要する敗血症性ショックでは、平均血圧 65 mmHgを目標とする。
・昇圧薬としては、ノルアドレナリンを第一選択薬とする。
・敗血症関連 ARDSでは、一回換気量 6 ml/kg、プラトー圧 30 cmH2O以下を目標とする。
→こちらの過去のブログ記事も参考に:入れる、締める、叩く!
㉖Transient smartphone blindness: Relevance to misdiagnosis in neurologic practice. (2017.1.18 published online)
2016年に NEJM誌に報告された transient smartphone blindnessについて。メカニズムは、一般人向けのサイトに詳しい。それ自体に害はないのだけれど、頭部MRIで小血管病巣と思われる白質病変が散在していたため、多発性硬化症と誤診されてしまったという報告。
㉗Ibrutinib monotherapy in relapsed/refractory CNS lymphoma: A retrospective case series. (2016.11.18 published online)
原発性中枢神経リンパ腫 (PCNSL) あるいは二次性中枢神経リンパ腫の対する Ibrutinibの後方視的ケースシリーズ 14名。いずれも、難治例 (12名) もしくは再発例 (2名)。最良の治療効果は、完全寛解が 3名、部分寛解が 4名。最終的には、5名死亡、6名が疾患活動性がありながら生存、3名が寛解を維持 (8, 8, 12ヶ月) であった。
㉘Improved Muscular Weakness During Asthma Exacerbation. (2017.1.3 published online)
48歳男性、小児期からの筋力低下で、針筋電図や、血清CKレベルなどは正常。喘息発作のため、アルブテロールおよびステロイドの吸入を行ったところ、筋力が改善し、階段をのぼったり、数 km歩いたりできるようになった。
診断は先天性筋無力症。DOK7変異による先天性筋無力症では、サルブタモール吸入 (10 mg/day) で症状が改善することが知られているようだ。機序は不明だが、MuSKシグナル経路の障害を軽減することによる終板構造の安定化が仮説と唱えられているらしい。
AbbVie社が初期アルツハイマー病患者と進行性核上性麻痺患者を対象に、抗タウ抗体 ABBV-8E12の第二相試験を開始するらしい。
進行の遅い患者も多いので、52週間進行を観察して有意差を示せるかなぁ・・・という気はするけれど、薬剤の機序的にとても期待している。
㉚Burnout, career satisfaction, and well-being among US neurologists in 2016. (2017.1.25 published online)
神経内科医の燃え尽き (burnout)、仕事満足度などについてのサーベイランス。米国神経内科学会の会員を対象とし、40.5%から回答を得られた。平均年齢は 51歳、65.3%が男性。少なくとも 60%が燃え尽きの症状を自覚していた。燃え尽きのリスクと関連していたのは、労働時間/週、夜間オンコール/週、外来患者数/週、事務仕事量だった。サポートスタッフ、仕事の裁量権、意義のある仕事、年齢、てんかんのサブスペシャリティがリスク低下と関連していた。アカデミア (Academic practice) の神経内科医は臨床 (clinical practice) の神経内科医と比較して、燃え尽き率が低く、満足度が高く、QOLも高かった。燃え尽きは、仕事満足度の低さと強く相関していた。
私はまだ燃えてすらいないダメ医者ヽ(´ー`)ノ
![]()