ステロイドと骨粗鬆症
神経疾患でステロイドを使う症例は結構あります。現在の私の外来でも、視神経脊髄炎 (NMO), 重症筋無力症、慢性炎症性多発根神経炎 (CIDP), Neuro-Sweet disease, Churg-Strauss症候群などの患者さんにステロイドの長期投与をしています。このようにステロイド投与をしている患者さんでは、投与後 3ヶ月以内に骨密度の減少が始まり、6ヶ月後ではその減少はピークに達します。そのため、骨粗鬆症対策が大事になってきます。しかし、神経内科医の間では、ステロイド性骨粗鬆症に対して議論になることは少ないのが現状なのではないかと思います。
「骨粗鬆症の予防と治療ガイドライン 2011年版」を紐解くと、116~117ページに「ステロイド性骨粗鬆症」の記載があり、「2010年現在,わが国では「ステロイド性骨粗鬆症の管理と治療のガイドライン2004年度版」が用いられており」とされますが、2004年のガイドラインではやや古い感は否めず、実際に新薬の開発に伴い薬物療法も変化してきています。
最近、アメリカリウマチ学会のガイドラインを読む機会があったのですが、非常にためになりました。無料でアクセスできて、内容もそれほど長くないのが素晴らしいところです。
American College of Rheumatology 2010 Recommendations for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis
JENNIFER M. GROSSMAN,1 REBECCA GORDON,2 VEENA K. RANGANATH,1 CHAD DEAL,3
LIRON CAPLAN,4 WEILING CHEN,1 JEFFREY R. CURTIS,5 DANIEL E. FURST,1 MAUREEN MCMAHON,1
NIVEDITA M. PATKAR,5 ELIZABETH VOLKMANN,1 AND KENNETH G. SAAG5
Arthritis Care & Research
Vol. 62, No. 11, November 2010, pp 1515–1526
DOI 10.1002/acr.20295
© 2010, American College of Rheumatology
このガイドラインの冒頭には、ガイドラインは絶対的なものではなく、個々の患者さんに応じて治療を決めるように、といった内容が書かれています。ガイドラインの立場を表した、非常に大事な文章だと思います (これを読むと、ガイドラインを訴訟の道具にすべきではありませんね)。
Guidelines and recommendations developed and/or endorsed by the American College of Rheumatology (ACR) are intended
to provide guidance for particular patterns of practice and not to dictate the care of a particular patient. The ACR
considers adherence to these guidelines and recommendations to be voluntary, with the ultimate determination regarding
their application to be made by the physician in light of each patient’s individual circumstances. Guidelines and recommendations
are intended to promote beneficial or desirable outcomes but cannot guarantee any specific outcome. Guidelines
and recommendations developed or endorsed by the ACR are subject to periodic revision as warranted by the evolution
of medical knowledge, technology, and practice.
以下、簡単に内容を紹介します。
①ステロイドを開始するときは、カルシウムとビタミン Dを補充することが推奨される。
Calcium and vitamin D supplementation counseling was recommended for all patients beginning glucocorticoid therapy. Vitamin D supplementation to achieve “therapeutic” levels of 25-hydroxyvitamin D, or dosages of 800–1,000 IU/day are 2 target dosing regimens; however, glucocorticoids can interfere with vitamin D absorption and may necessitate a higher supplementation dose to achieve therapeutic levels (97).
②閉経後女性、50歳以上の男性にステロイドを開始するときは、FRAXにより骨折リスクを評価して、治療を決定する。
・FRAXのサイトは下記。サイト上部にある「計算ツール」タブから、患者の人種を選べる (骨折リスクには人種差がある)。
FRAX
・ FRAXによる 10年間の骨折確率から、骨折リスクを ” ≦10% low risk, 10~20% medium risk, 20% < high risk” とする。
・下記フローチャートに則り、治療を決定する。
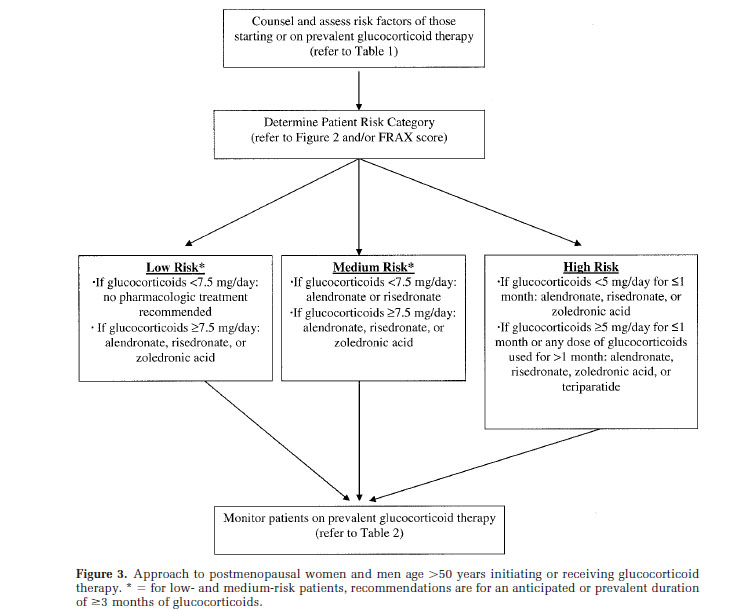
Approach to postmenopausal women and men age > 50 years
※薬物名に関しては次の通り
alendronate: フォサマック、ボナロン, risedronate: ベネット、アクトネル, teriparatide フォルテオ, zoledronic acid: ゾメタ (※ゾメタは、日本においては骨粗鬆症では保険適応外。内分泌学会から要望が出されたが却下された模様)
③閉経前女性および 50歳未満の男性にステロイドを開始するときは、下記フローチャートに従う。
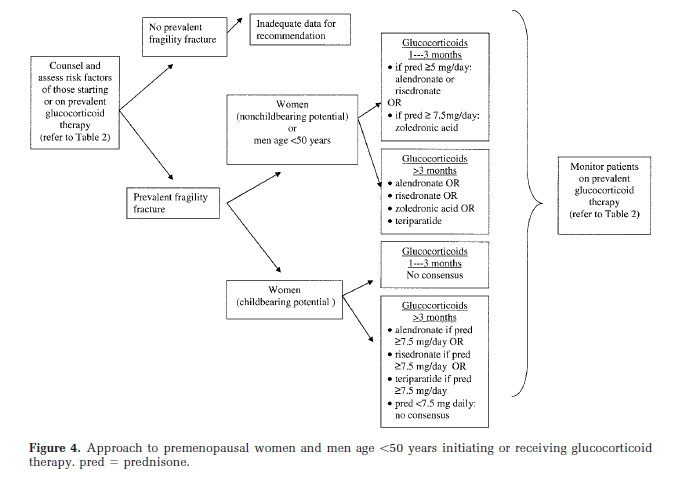
Approach to premenopausal women and men age < 50 years
![]()